Alcohol
Last Modified 03/08/2023 15:44:56
Share this page
Further information relating to young people can be found in the Alcohol use in children and young people section.
An estimated 10.8 million adults in England are drinking at levels that pose some risk to their health and 1.6 million may have some level of alcohol dependence. Although not all of these need specialist treatment, a proportion of them will benefit from a brief intervention. Alcohol is the third leading risk factor for death and disability after smoking and obesity and has been identified as a causal factor in more than 60 medical conditions including cirrhosis of the liver, heart disease, depression, pancreatitis and stroke as well as a number of cancers. Alcohol can be a long-term condition and dependent individuals may experience many health problems and are frequent users of health services. Excessive alcohol consumption is a major cause of preventable premature death.
Alcohol misuse impacts not just on the drinker but also those around them. Children affected by parental alcohol misuse are more likely to have physical, psychological and behavioural problems. Parental alcohol misuse is strongly correlated with family conflict and with domestic violence (DV) and abuse. This poses a risk to children of immediate significant harm and of longer-term negative consequences.1
Despite clubs, pubs etc. closing during national COVID-19 lockdowns, the total amount of alcohol released for sale during the pandemic was still similar to the pre-pandemic years, which suggests people were drinking more at home. Comparing March 2020 and March 2021, there was a 58.6% increase of people reporting that they were drinking at increasing and higher-risk levels (50 units a week for men, 35 units a week for women). The hidden harm experience of children and young people who were living with, and impacted by, parental alcohol use (and potentially increased levels of DV) throughout lockdowns should be considered.
The Office for Health Improvements and Disparities (OHID) produced a COVID-19 Health Inequalities Monitoring for England (CHIME) tool which reports on trends in alcohol purchasing and consumption throughout the pandemic as well as on trends in hospital admissions and mortality.2
Data presented in CHIME shows the prevalence of increasing and higher risk drinking increasing sharply at the start of the pandemic for both males and females, and while rates have come down they are not back to pre-pandemic levels.
Figure 1: prevalence of increasing and higher risk drinking in England (to December 2021)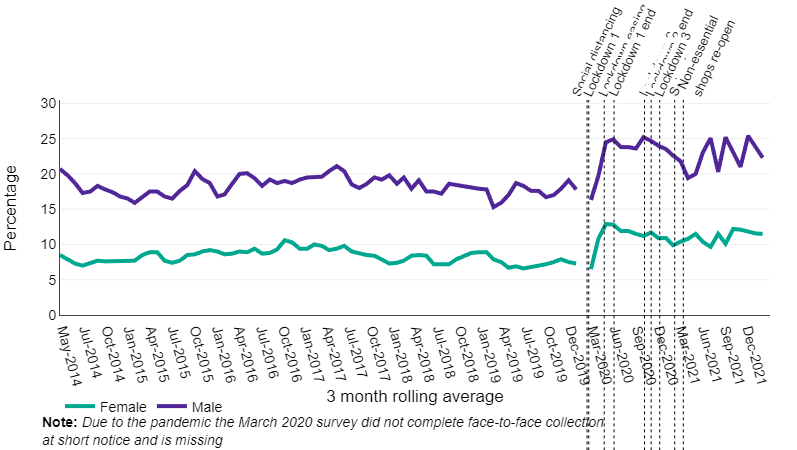 Source: Office for Health Improvement & Disparities (OHID), COVID-19 Health Inequalities Monitoring for England (CHIME)
Source: Office for Health Improvement & Disparities (OHID), COVID-19 Health Inequalities Monitoring for England (CHIME)
The data also shows that alcohol-specific hospital admissions initially decreased sharply as the pandemic hit before rising quite quickly again. Rates are now similar to pre-pandemic levels. However, alcohol-specific mortality across England shows a more concerning picture with significantly higher than average mortality rates over the course of 2020, 2021 and into 2022.
Figure 2: monthly trend in mortality for all alcohol-specific conditions in England – all persons
Source: OHID, COVID-19 Health Inequalities Monitoring for England (CHIME)
The consequences of alcohol misuse are worse in the North West of England than other regions of the UK, and Blackpool has high levels of alcohol-related harm (health, disorder, violence) for the size of the population.
Blackpool has a thriving and vibrant night-time economy (NTE). It is an important part of the character of the town and attracts many visitors, and the economy centres round entertainment premises licensed to sell alcohol. The contribution this industry makes to the economic wellbeing of the town is significant and it is also a source of work for many people. Almost half of all employment in Blackpool is driven by the NTE with a rate of 48.8% in comparison to the NTE employment rate for England and Wales at 35% (this includes all activity that feasibly operates at night).
While there are economic benefits for the town, the health and negative social impacts can be damaging. Tourists contribute a significant amount to the NTE, especially during the summer. This affects crime statistics, with tourists featuring as both victims and offenders. Blackpool has the highest number of licensed premises in Lancashire with 2021 figures showing 1,346 licensed premises (approximately one for every 80 adults), including 117 pubs and 144 off-licences; a very high number of those licensed premises are in the town centre and the inner wards, which also experience higher levels of deprivation.
A busy NTE has its associated problems. The effects of alcohol and drugs and the concentration of people are two factors, among others, which can spark aggression and high demand for emergency services. Alcohol is a common factor in crime, with 3,239 alcohol-related crimes in Blackpool (Jan-21 to Dec-21) an increase of 28% compared with the previous 12-month period. Just over a third (34%) of violence against the person offences in the town centre are linked to alcohol.3
The most effective strategies to reduce alcohol-related harm from a public health perspective include, in rank order, price increases, restrictions on the physical availability of alcohol, restrictions on alcohol advertising, licensing, brief interventions with at-risk drinkers, and treatment of drinkers with alcohol dependence.4
Alcohol-related harm is largely determined by the volume of alcohol consumed and the frequency of drinking occasions. As such, the risk of harm is directly related to levels and patterns of consumption. However, there can be a considerable lag between alcohol consumption and alcohol-related harm, particularly for chronic conditions where the lag can be many years. In England a quarter of the population are drinking at above low risk levels so may benefit from some level of intervention. Harm can be short-term and instantaneous, due to intoxication or long-term, from continuous exposure to the toxic effect of alcohol or from developing dependence
To keep health risks from alcohol to a low level it is safest not to drink more than 14 units a week on a regular basis. The Chief Medical Officers' guidelines for both men and women are that:5
-
- To keep health risks from alcohol to a low level it is safest not to drink more than 14 units a week on a regular basis.
- If you regularly drink as much as 14 units per week, it is best to spread your drinking evenly over three or more days.
- If you have one or two heavy drinking episodes a week, you increase your risks of death from long-term illness and from accidents and injuries.
- The risk of developing a range of health problems (including cancers of the mouth, throat and breast) increases the more you drink on a regular basis.
- If you wish to cut down the amount you drink, a good way to help achieve this is to have several drink-free days each week.
Figure 3 gives estimates for the number of the population drinking at increasing and higher risk levels. The more units regularly consumed per day increases the risk factor, whilst binge drinkers could drink at any level normally with an occasional binge. Dependent drinkers are predominantly a subset of either increasing risk or higher risk drinkers, however recovering drinkers could be abstinent but remain dependent. The risk of harm from alcohol is directly related to levels and patterns of consumption.
Figure 3: increasing and higher risk drinkers in England, 2014
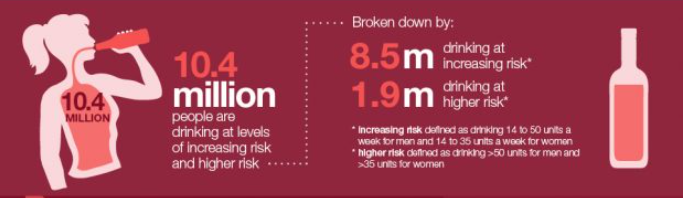 Source: PHE, Health Matters: Identifying and offering brief advice to tobacco and alcohol users, March 2019
Source: PHE, Health Matters: Identifying and offering brief advice to tobacco and alcohol users, March 2019
Figure 4: Patterns of alcohol consumption for Blackpool and England (%)
| | Blackpool | England |
|---|
| Adults who abstain from drinking |
17.3% |
16.2% |
| Adults drinking less than 14 units per week |
60.0% |
61.0% |
| Adults drinking more than 14 units per week |
22.7% |
22.8% |
| Source: PHE/NDTMS, Alcohol commissioning support pack, 2022-23 |
Estimated data from the Health Survey for England 2015-18 suggests that the consumption of alcohol across Blackpool is similar to the England average. However, in the UK, less affluent people experience a higher rate of alcohol-related health problems, despite people in different socioeconomic groups having similar alcohol consumption levels. This is known as the ‘alcohol harm paradox’.6
Drinking combined with other health-challenging behaviours, such as smoking or having a poor diet, has been found to multiply the risk of developing conditions like alcoholic liver disease and some cancers, compared to doing them separately or not at all. Less affluent drinkers are more likely to have more health-challenging behaviours, compared to their more affluent counterparts. This multiplied risk may explain the difference in harm, despite the different groups drinking similar amounts.
-
- Data from the Local Alcohol Profiles for England shows that Blackpool has more than double the estimated number of dependent drinkers than is seen nationally: 3.8% compared to 1.4% (2014/15).
Blackpool has by far the most licensed premises of any district in Lancashire-14. A fifith (1,346) of over 6,700 licensed premises in Lancashire are located within the town.
- Almost half (49%) of Blackpool's full licenses are held by hotels.
- There are 144 (11%) off-licences and 117 (9%) pubs.
- Almost two thirds (850) of Blackpool's licensed premises are located within Bloomfield, Claremont and Talbot.
- Excluding the three town centre wards, numbers of licensed premises range from 145 in Waterloo to 6 in Highfield.
Figure 5: Number of licensed premises in Blackpool as at December 2021
| | Hotel | Off-license | Restaurant* | Pub | Late night refreshment house | Members club/night club | Convenience store/ supermarket | Takeaway | Other | Total | % in ward |
|---|
| Anchorsholme |
2 |
5 |
1 |
|
1 |
|
2 |
|
2 |
13 |
1.0% |
| Bispham |
9 |
3 |
9 |
4 |
2 |
1 |
2 |
|
2 |
32 |
2.4% |
| Bloomfield |
206 |
17 |
12 |
20 |
20 |
3 |
3 |
5 |
10 |
296 |
22.0% |
| Brunswick |
|
6 |
|
3 |
2 |
2 |
|
|
1 |
14 |
1.0% |
| Claremont |
100 |
19 |
17 |
17 |
15 |
14 |
1 |
8 |
8 |
199 |
14.8% |
| Clifton |
1 |
9 |
2 |
2 |
2 |
|
3 |
1 |
1 |
21 |
1.6% |
| Greenlands |
|
4 |
1 |
1 |
2 |
|
1 |
|
1 |
10 |
0.7% |
| Hawes Side |
|
7 |
1 |
1 |
4 |
2 |
1 |
|
|
16 |
1.2% |
| Highfield |
|
4 |
|
2 |
|
|
|
|
|
6 |
0.4% |
| Ingthorpe |
|
3 |
3 |
2 |
|
|
2 |
1 |
4 |
15 |
1.1% |
| Layton |
|
6 |
1 |
2 |
1 |
2 |
2 |
|
2 |
16 |
1.2% |
| Marton |
1 |
5 |
2 |
3 |
|
2 |
|
|
6 |
19 |
1.4% |
| Norbreck |
1 |
1 |
1 |
2 |
|
4 |
|
|
|
9 |
0.7% |
| Park |
|
1 |
|
|
|
1 |
1 |
|
6 |
9 |
0.7% |
| Squires Gate |
5 |
4 |
12 |
2 |
2 |
3 |
1 |
|
2 |
31 |
2.3% |
| Stanley |
|
4 |
2 |
3 |
|
5 |
3 |
|
5 |
22 |
1.6% |
| Talbot |
186 |
14 |
60 |
35 |
19 |
14 |
5 |
5 |
17 |
355 |
26.4% |
| Tyldesley |
|
6 |
1 |
1 |
1 |
1 |
2 |
1 |
|
13 |
1.0% |
| Victoria |
|
11 |
2 |
1 |
5 |
3 |
1 |
|
2 |
25 |
1.9% |
| Warbreck |
52 |
6 |
2 |
5 |
6 |
|
4 |
2 |
3 |
80 |
5.9% |
| Waterloo |
96 |
9 |
11 |
11 |
6 |
2 |
1 |
2 |
7 |
145 |
10.8% |
| Blackpool |
659 |
144 |
140 |
117 |
88 |
59 |
35 |
25 |
79 |
1,346 |
100% |
| *includes restaurant/takeaway, restaurant/bar and restaurant/café Source: Lancashire Insight, MADE Partners data, December 2021 |
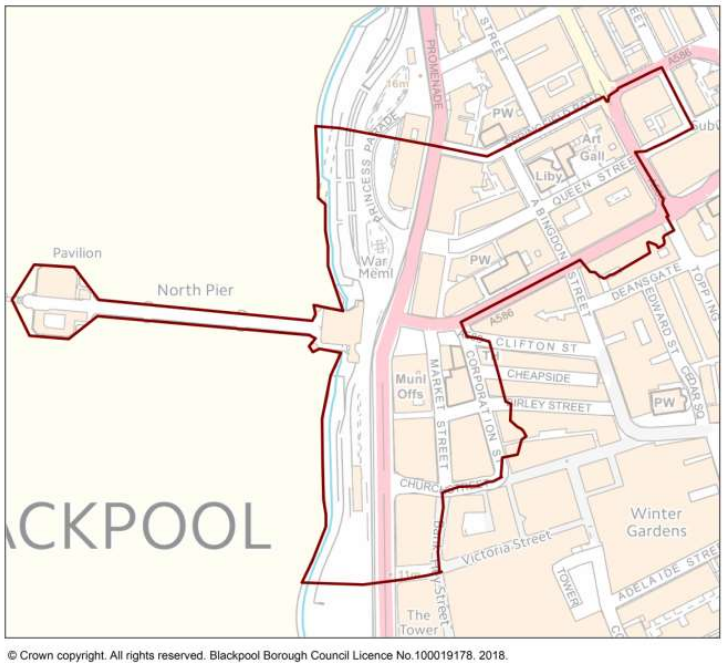
The number, type and density of premises selling alcohol in a particular area can lead to serious problems of nuisance or disorder. In these circumstances the impact of the premises taken as a whole can be far greater than that arising from individual premises. In most cases it would be impossible to identify individual premises as being the sole cause or major contributing factor. For this reason, the licensing authority in Blackpool has created a town centre assessment area and an off-licence saturation area policy, Blackpool Cumulative Impact Assessment 2021. The area covered by the town centre saturation area is shown in Figure 6.
The policy applies to applications including the sale or supply of alcohol on the premises. The effect of the policy is to create a rebuttable presumption that applications will be refused. To rebut this presumption an applicant would be expected to show that the operation of the premises will not add to the cumulative impact already being experienced.
This policy does not act as an absolute prohibition on the granting of new licences however the policy will only be overridden in genuinely exceptional cases where the applicant can demonstrate that the granting of the application will not undermine the policy and the reasons for it. An application is not likely to be classed as exceptional merely on the ground that the premises have been or will be operated within the terms of its licence or that they are/will be well managed. This is to be expected of any application.
Despite the adoption of such a policy, if no representations are received from responsible authorities, the application must be granted in terms consistent with the operating schedule.
Figure 6: town centre assessment area
Off-licence saturation policy
The off-licence saturation policy intends to promote a saturation zone within Blackpool in areas where crime and disorder is more prevalent and alcohol-related health statistics are high. The area to which this off-licence saturation policy will apply includes Claremont, Bloomfield and Talbot wards in their entirety as well as part of Brunswick ward and Waterloo ward. For the avoidance of any doubt, premises located along both sides of the highway where the boundary line is drawn are considered to be included in the saturation area.
Alcohol is a major cause of ill health; it causes and contributes to a wide range of serious health problems, accidents and deaths. The health effects of alcohol can be acute, for example poisoning or injury; and chronic (long term), for example liver cirrhosis, cardiovascular disease or female breast cancer. An analysis of 67 risk factors and risk factor clusters for death and disability found that alcohol is the third leading risk factor for death and disability after smoking and obesity.1 In most cases, the relationship between alcohol and disease is 'dose-dependent' - the more alcohol consumed, the greater the risk of disease.
 Source: PHE, Health matters: harmful drinking and alcohol dependence, January 2016
Source: PHE, Health matters: harmful drinking and alcohol dependence, January 2016
Mortality and hospital admissions due to alcohol
Alcohol consumption is a contributing factor to hospital admissions and deaths from a diverse range of conditions and there are a number of definitions used to describe alcohol mortality and admissions.
Definitions
-
- The term 'alcohol-specific conditions' refers to conditions caused wholly by the use of alcohol including alcohol-induced behavioural disorders and alcohol-related liver cirrhosis. Alcohol-related conditions are wholly or partially caused by alcohol.
- Alcohol-related mortality refers to deaths with an alcohol attributable fraction based on the underlying cause of death (including ethanol or methanol poisoning and the toxic effects of alcohol).
- Broad definition: A measure of hospital admissions where either the primary diagnosis (main reason for admission) or one of the secondary (contributory) diagnoses is an alcohol-related condition. This represents a broad measure of alcohol-related admissions but is sensitive to changes in coding practice over time.
- Narrow definition: A measure of hospital admissions where the primary diagnosis (main reason for admission) is an alcohol-related condition. This represents a narrower measure. Since every hospital admission must have a primary diagnosis it is less sensitive to coding practices but may also understate the part alcohol plays in the admission.
- In general, the broad measure gives an indication of the full impact of alcohol on hospital admissions and the burden placed on the NHS. The narrow measure estimates the number of hospital admissions which are primarily due to alcohol consumption and provides the best indication of trends in alcohol-related hospital admissions.
Figure 7 shows that Blackpool is significantly worse than the England average on all alcohol mortality indicators and is the worst in the country for some measures.
Figure 7: Alcohol and mortality Source: OHID, Local Alcohol Profiles for England, July 2023
Source: OHID, Local Alcohol Profiles for England, July 2023
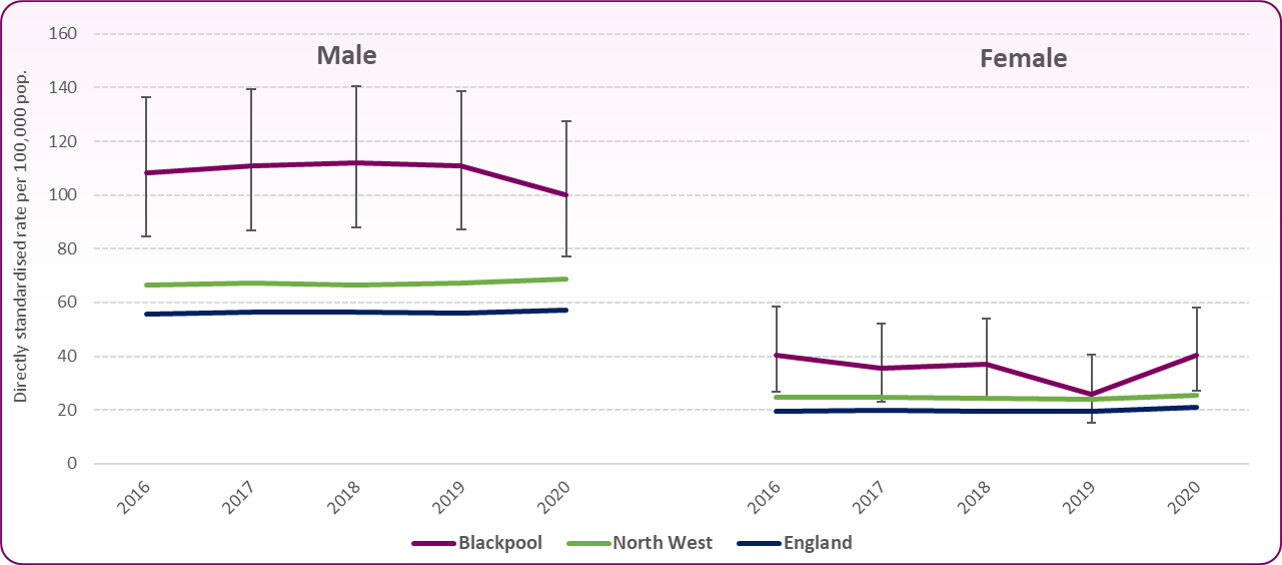
Figure 8 shows alcohol-specific mortality for males and females in Blackpool compared to the North West region and England as a whole. For males the rate in Blackpool had been showing a gradual decline until 2012-14 but did begin to increase again. However, the mortality rate has been static for the last three years and is currently 39.2 per 100,000. This is approximately two and a half times higher than the national average of 14.9 per 100,000. For females, alcohol-specific mortality had been increasing since 2010-12 although the rate fell in 2017-19 to 15.5 per 100,000. This compares to the England rate of 7.1. The rates are still significantly higher than national averages for both males and females.
Figure 8: Trend in alcohol-specific mortality for males and females, Blackpool, North West and England
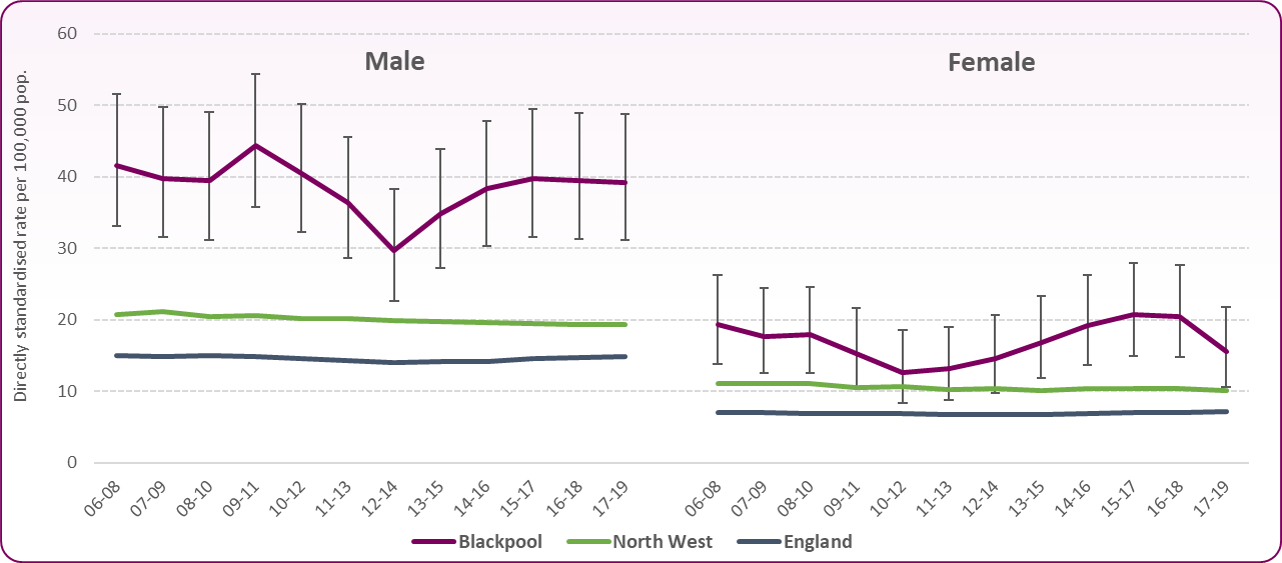 Source: OHID Local Alcohol Profiles for England, February 2022
Source: OHID Local Alcohol Profiles for England, February 2022
Alcohol-related mortality includes conditions wholly-attributable and partially-attributable to alcohol. Figure 9 shows the trend in alcohol-related mortality for males and females in Blackpool compared to the North West and England as a whole. The male and female mortality rates have been significantly higher than England for a number of years.*
Figure 9: Trend in alcohol-related mortality for males and females, Blackpool, North West and England
 Source: OHID Local Alcohol Profiles for England, February 2022*Due to the revision of official population estimates (mid-2012 to mid-2020) the trend data are not available using the most recent data (2021) and the 2021 data cannot be compared to previous years.
Source: OHID Local Alcohol Profiles for England, February 2022*Due to the revision of official population estimates (mid-2012 to mid-2020) the trend data are not available using the most recent data (2021) and the 2021 data cannot be compared to previous years.
Alcohol misuse is estimated to cost the NHS about £3.5 billion per year and society as a whole £21 billion annually.1 Hospital admissions can be a result of regular alcohol use above lower-risk levels; around three-quarters of the cost to the NHS is incurred by people who are not alcohol dependent, but whose alcohol misuse causes ill health.
Alcohol-specific admissions
-
- There were 1,765 alcohol-specific hospital admissions to Blackpool residents in 2021/22: 69% male, 31% female.
- The alcohol-specific admission rate is significantly higher than the national average for males and females.
- Blackpool has significantly higher rates of alcohol-specific admissions for people with 0, 1, 2 or 3 previous admissions in the preceding 24 months indicating there is a pattern of frequent attendance at hospital in Blackpool that is significantly worse than England as a whole.
- For young people aged under 18 years, the trend in admissions has generally been falling and the rate is now similar to the England average. There were only 20 admissions over the three-year period 2018/19-2020/21 in this age group (22.9 per 100,000, England 29.3).
Figure 10: trend in alcohol-specific hospital admissions, all ages and age under 18 years, Blackpool, North West and England*
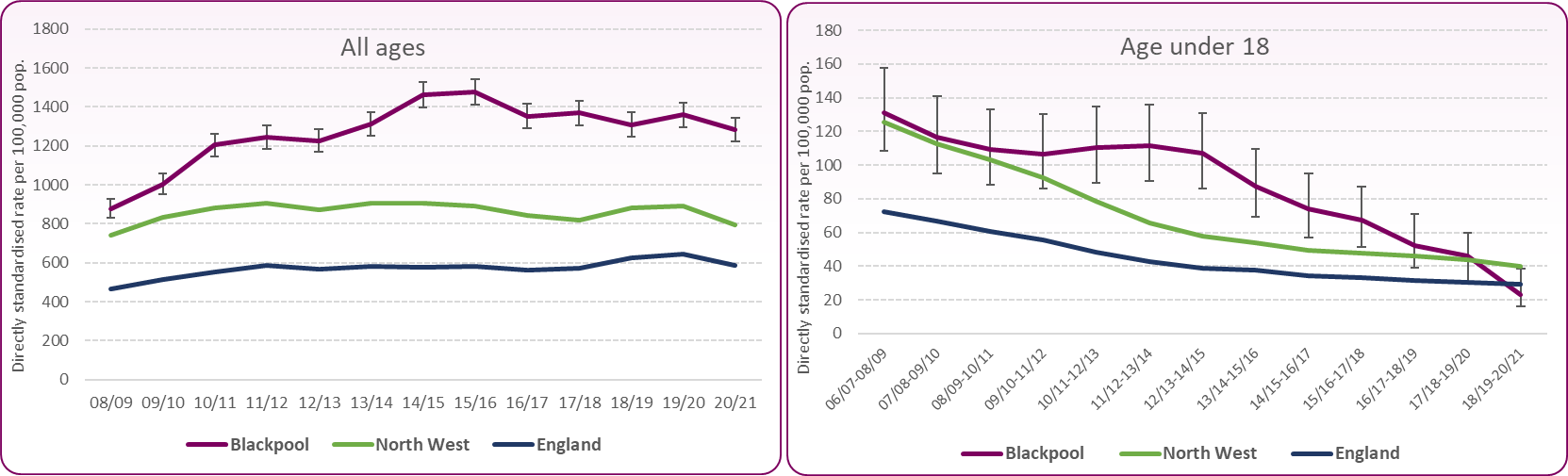 Source: OHID Local Alcohol Profiles for England, February 2022*Due to the revision of official population estimates (mid-2012 to mid-2020) the trend data are not available for the most recent data (2021/22) and this data cannot be compared to previous years.
Source: OHID Local Alcohol Profiles for England, February 2022*Due to the revision of official population estimates (mid-2012 to mid-2020) the trend data are not available for the most recent data (2021/22) and this data cannot be compared to previous years.
Alcohol-related admissions
- Men account for the majority (72%) of alcohol-related admissions (broad definition). This reflects a higher level of harmful drinking among men compared to women overall.
- There were 3,917 alcohol-related (broad definition) hospital admissions of Blackpool residents in 2021/22, approximately 7.5% of all admissions
- Rates of alcohol-related (narrow) hospital admissions (2021/22) are significantly higher than the England average, with the rate for males at 990 (England 664 per 100,000). The rate for females is 527 (England 341 per 100,000). As with the alcohol-specific admissions, trend data are not available for the 2021/22 rates so comparisons cannot be made with previous years.
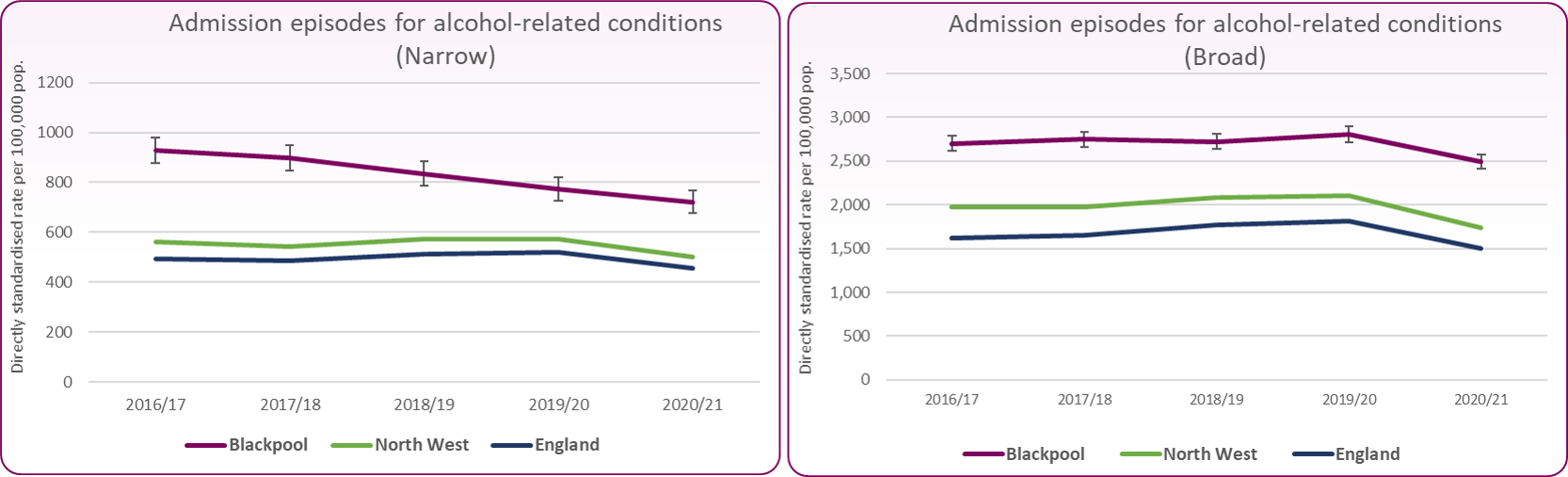
Looking at the 2020/21 data in figure 11 below, the ‘narrow’ definition shows a declining trend which is positive and the generally static ‘broad’ definition also shows a decline during 2020/21 in line with the regional and national picture but some of this decline was due to fewer admissions because of COVID-19. Alcohol-related conditions still place a significant burden on the NHS and the population revisions and subsequent trend data, when released, will provide a fuller picture.
Figure 11: trends in alcohol-related hospital admissions, persons, (narrow and broad definitions)
 Source: PHE Local Alcohol Profiles for England, February 2022
Source: PHE Local Alcohol Profiles for England, February 2022
Hospital admissions by condition
The conditions shown in the graphs below have been selected because of their prevalence or because they are of particular concern for some local areas and may be the focus of wider strategic action.7 As males are more likely to experience the consequences of alcohol consumption, the indicators here (2021/22) are provided by sex in order to reflect this differential harm.8
The final indicator looks at the incidence rate of cancer by sex. This is based on data from the National Cancer Registration and Analysis Service (NCRAS) as this is more indicative of the incidence of alcohol-related cancer.
-
- Alcohol-related cardiovascular disease, and mental and behavioural disorders due to alcohol (broad) are the most common conditions.
- Males account for most of these two alcohol-related conditions, 84% and 71% respectively
- Males also account for 70% of alcoholic liver disease admissions and 86% of alcohol-related unintentional injury.
- Only admissions for intentional self-poisoning by and exposure to alcohol is evenly split, 50% male, 50% female.
Figures 12 - 14 show hospital admission episodes for selected alcohol-related conditions in England, North West and Blackpool in 2020/21
Figure 12: admission episodes for alcohol-related cardiovascular disease and alcoholic liver disease (2021/22) Source: OHID Local Alcohol Profiles for England, August 2023 Figure 13: admission episodes for mental and behavioural disorders due to the use of alcohol, and intentional self-poisoning by alcohol (2021/22)
Source: OHID Local Alcohol Profiles for England, August 2023 Figure 13: admission episodes for mental and behavioural disorders due to the use of alcohol, and intentional self-poisoning by alcohol (2021/22)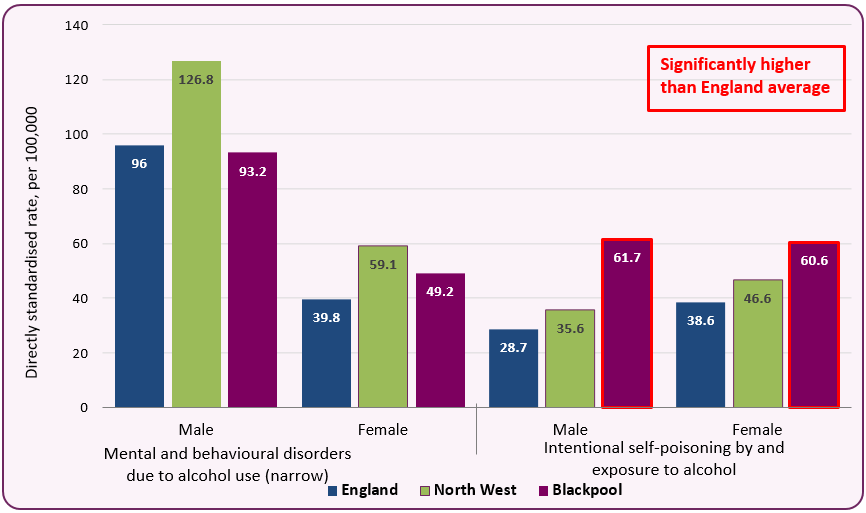 Source: OHID Local Alcohol Profiles for England, July 2023 Figure 14: admission episodes for alcohol-related unintentional injuries (2021/22) and the incidence rate of alcohol-related cancer (2017-19)
Source: OHID Local Alcohol Profiles for England, July 2023 Figure 14: admission episodes for alcohol-related unintentional injuries (2021/22) and the incidence rate of alcohol-related cancer (2017-19)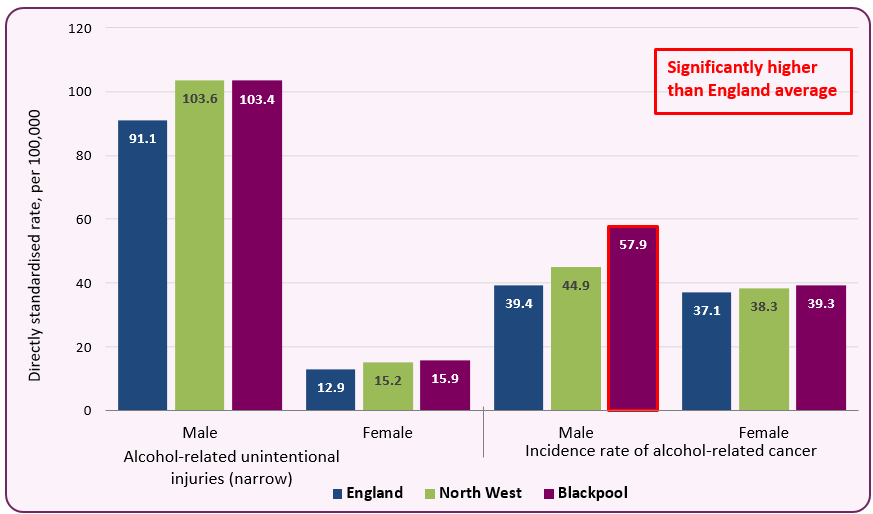 Source: OHID Local Alcohol Profiles for England, August 2023
Source: OHID Local Alcohol Profiles for England, August 2023
Figure 15 shows alcohol-attributable hospital admissions by ward in Blackpool. All wards, except Norbreck, have higher admission rates than the national average. This shows the harm resulting from alcohol misuse is more concentrated in the most disadvantaged areas of Blackpool. Harmful use of alcohol affects the most vulnerable groups in society - those in the lowest income bracket and those experiencing the highest levels of deprivation. Even though lower socioeconomic groups often report lower levels of average consumption, they experience greater or similar levels of alcohol-related harm.
Figure 15: alcohol-attributable hospital admissions (broad definition) by ward, 2016/17-20/21
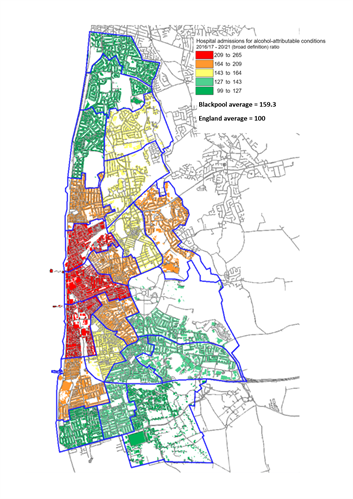 Source: OHID, Local Health Profiles, August 2023
Source: OHID, Local Health Profiles, August 2023
Frequent hospital admissions
Information on individuals who are frequently admitted to hospital for alcohol-specific conditions gives an indication of the number of drinkers who place a heavy burden on health services and, very often, on social housing and criminal justice services. The fact that these people are experiencing ongoing alcohol-specific ill health suggests that they may not have had contact with treatment services, or if they have, it is unlikely that services have engaged with them for long enough for them to achieve sustained abstinence. Figure 16 shows the number (and rate) of frequent alcohol-specific admissions for Blackpool compared with England. The rate of three or more previous admissions by individuals in Blackpool is almost double the national average.
Figure 16: individuals with alcohol-specific hospital admissions in 2020/21 and number of admissions in the preceding 24 months
| | England | Blackpool |
|---|
| | Rate per 100,000 | Number of admissions | Rate per 100,000 |
|---|
| No previous admissions |
228 |
705 |
645 |
| 1 previous admission |
69 |
225 |
206 |
| 2 previous admissions |
36 |
90 |
82 |
| 3 or more previous admissions |
85 |
170 |
156 |
| Source: PHE, Adults - alcohol commissioning support pack 2022-23: key data |
Whilst the majority of young people do not use alcohol or drugs, and most of those who do are not dependent, drug and alcohol misuse can have a major impact on young people's education, their health, their families and their long-term chances in life. Further information on young people and alcohol-related harm in Blackpool is available in the Alcohol use in children and young people section.
Alcohol-related crime makes up a substantial portion of violent offences, 39% in England and Wales in 2017/18, and is estimated to cost between 1.3 and 2.7% of the UK annual GDP (£21-£52 billion), according to a 2016 Public Health England report. Alcohol also places a significant burden on the emergency services – three-quarters of police and half of ambulance respondents have been injured in alcohol-related incidents – while research has also highlighted the role of alcohol in domestic violence, sexual assault, child abuse, and violent crime including murder.9
Alcohol is too often a precursor and catalyst for crime and disorder in Blackpool in addition to creating health and safety issues in the wider community. Blackpool is a local authority containing some of the most deprived areas in Lancashire and England and there is a correlation between Blackpool's areas of deprivation and hotspots for violent crime, domestic abuse and criminal damage; all associated with alcohol abuse to some degree.
Visitors to Blackpool swell the local population significantly during the summer months, and although they make a huge contribution to the local economy, including a substantial 'night time economy', they also contribute to the local crime statistics as victims or offenders. Although rates have fallen, in part due to the coronavirus pandemic, Blackpool still has the highest rate of alcohol-related crime in Lancashire. Figure 17 shows the trend in alcohol related crimes across Blackpool and Lancashire, while figure 18 shows the differences within Blackpool.
-
- There were over 2,200 alcohol-related crimes in Blackpool in 2020/21, approximately a fifth of Lancashire's total of 11,559.10
- Alcohol-related crime has halved in Blackpool and across Lancashire since 2018/19.
- While rates have fallen across Blackpool, they are still twice the Lancashire average; 16.4 per 1,000 population compared to 7.6.
- Alcohol-related violence makes up approximately 60% of all alcohol-related crime.
- Almost half (46%) of alcohol-related crime is concentrated in three wards in central Blackpool; Bloomfield, Claremont and Talbot, reflecting the most disadvantaged areas and the night time economy within the town (figure 18).
Figure 17: trend in the rates of alcohol-related violence and 'other' alcohol-related crimes in Lancashire-14 and Blackpool
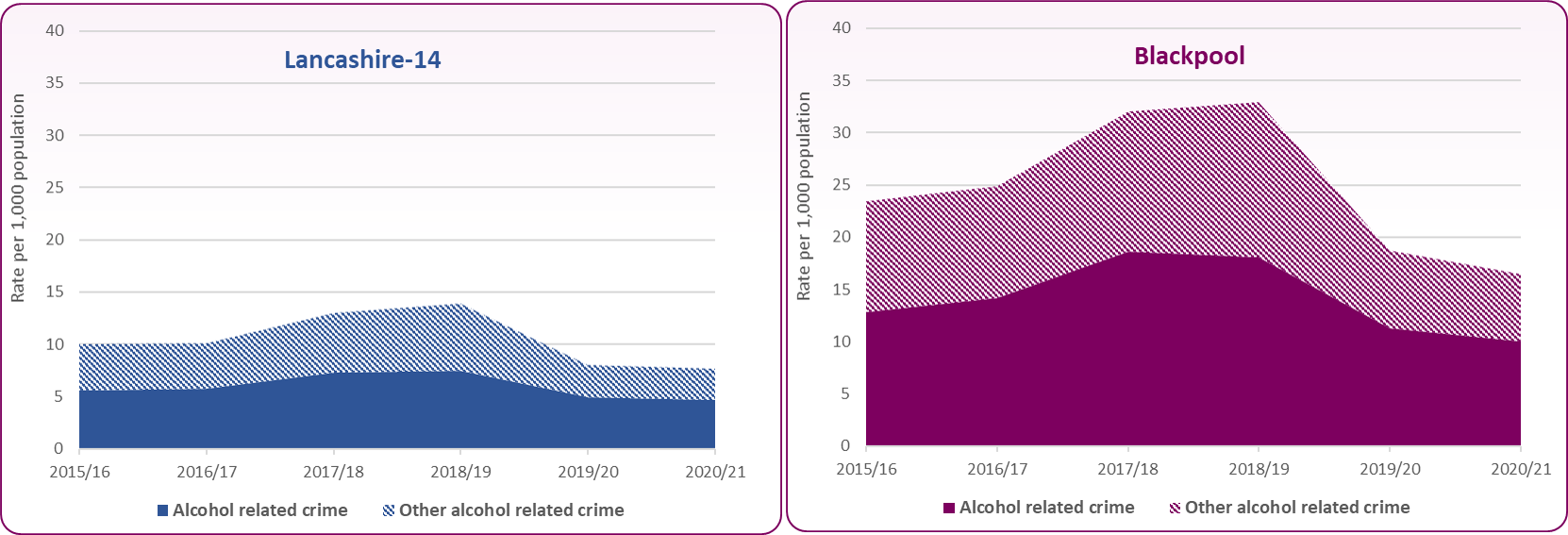 Source: Lancashire Insight, MADE Partners data, March 2022
Source: Lancashire Insight, MADE Partners data, March 2022
Figure 18: rates of all alcohol-related crime by ward, 2020/21
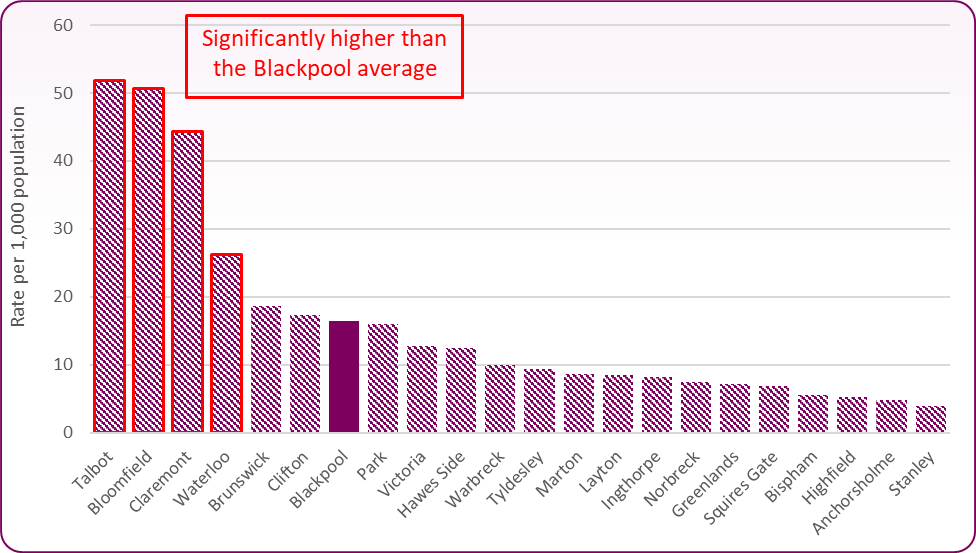 Source: Lancashire Insight, MADE Partners data, March 2022
Source: Lancashire Insight, MADE Partners data, March 2022
There is a strong relationship between alcohol and domestic abuse, violence and sexual assault. Whilst alcohol should not be used as an excuse for those who perpetrate violence and abuse, neither should its influence be ignored. Alcohol misuse is consistently found in a high proportion of those who perpetrate domestic abuse and sexual assault, and it has been found that within intimate relationships where one partner has a problem with alcohol or other substances, domestic abuse is more likely to occur.11 Blackpool has high levels of domestic violence compared to Lancashire as well as high numbers of dependent drinkers.
Information on individuals who are in contact with structured alcohol treatment services is available from the National Drug Treatment Monitoring System (NDTMS) which collects, collates and analyses data from and for those involved in the drug and alcohol sector.
Horizon Support Service
Horizon is the integrated drug and alcohol treatment service for residents of Blackpool. Delphi and Renaissance are the organisations that provide Horizon’s treatment services for alcohol. The service provides planned care and integrated community based treatment for drug and alcohol clients. Specifically, unstructured and structured interventions are available for people presenting with alcohol problems and one to one interventions are complemented by a variety of group work programmes. Treatment options will depend upon the needs and complexities of each client. Alcohol clients can receive brief advice and interventions within a number of community settings and are referred into more intensive support at the main treatment centre if required. Structured treatment is care planned and consists of community based psychosocial interventions and clinical treatment. Community detoxification and rehabilitation are also available to clients who would benefit from these approaches. Specific police and probation programmes are delivered to people where alcohol is related to offending behaviours and these include alcohol interventions to support treatment and offender prevention.
There was a small dip in alcohol clients over the period of COVID-19 restrictions shown in the local NDTMs report.12 These are people that need a specialist service. In-patient detoxification also decreased during COVID-19 restrictions due to a reduction in the number of beds available to allow social distancing. This number has now risen to above pre-pandemic levels.
Numbers in treatment for alcohol however remain low in comparison to local prevalence estimates and rates of unmet need for alcohol treatment. There are an estimated 3,867 dependent drinkers living in Blackpool, a rate of 3.5% which is more than 2.5 times higher than the England average of 1.4%. This leads to an estimate that 87% of dependent drinkers are not in treatment in Blackpool, (this estimate only counts those in treatment for alcohol only or alcohol and a non-opiate drug). Estimated local unmet need is thus higher than the national estimate of 82%.13
-
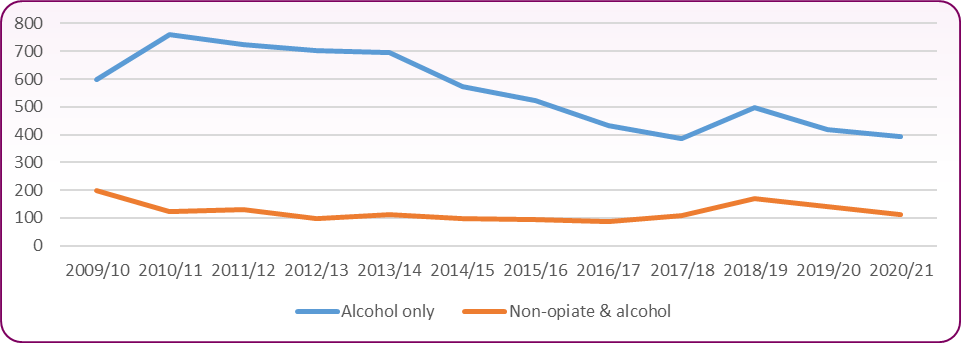
- The total number of clients in treatment in Blackpool in 2020/21 with an alcohol dependence, alone or in combination with any other drug, was 693. Of these, 394 were 'alcohol only' clients.
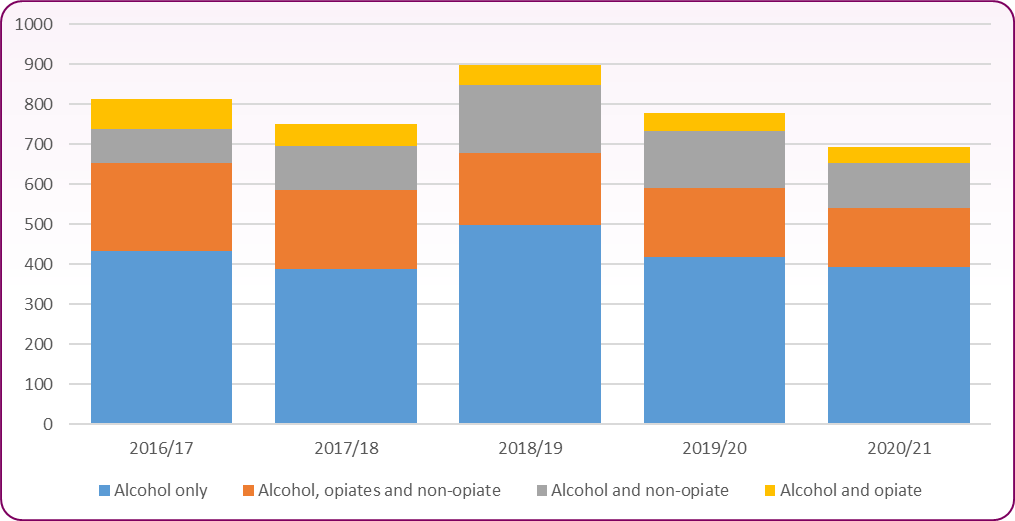
Figure 19 presents numbers of ‘alcohol only’ and ‘non-opiate and alcohol’ clients in treatment over the last 12 years and highlights the long term declining trend in the numbers of ‘alcohol only’ clients. Figure 20 shows the total number of clients in treatment who have a problem with alcohol.
Figure 19: trend in number of 'alcohol only' and 'non-opiate and alcohol' clients in treatment - Blackpool residents
 Source: PHE, Adults - alcohol commissioning support pack 2022-23: key data
Source: PHE, Adults - alcohol commissioning support pack 2022-23: key data
Figure 20: number of clients in treatment who have a problem with alcohol - Blackpool residents
 Source: PHE, Adults - alcohol commissioning support pack 2022-23: key data
Source: PHE, Adults - alcohol commissioning support pack 2022-23: key data
Clients in alcohol treatment
During 2020/21 the gender and age split of those accessing treatment was broadly in line with the national picture for treatment services.
-
- Of the 394 'alcohol only' clients in Blackpool in 2020/21, 60% were male and 40% were female.
The Health Survey for England 2018 (HSE) found that twice as many men as women drank at increasing or higher risk levels (anything over 14 units weekly). Higher risk drinkers, the group most likely to need treatment, are defined as males drinking over 50 units weekly and females drinking over 35 units weekly; 62.5% of this group were male and 37.5% were female. In other words, the gender split seen entering our treatment service is broadly in keeping with the gender split we would expect in the population of highest risk drinkers locally. The HSE also shows that the proportion of those drinking over 14 units a week increases from the age of 16 up to the age of 64 and then declines.14 The proportion of those entering Blackpool treatment services by age band is also broadly consistent with this national population picture.
Figure 21: number of clients entering 'alcohol only' treatment services by age group: 2020/21
| | Blackpool | England |
|---|
| Age | No. | % of all in treatment | Male (%) | Female (%) | No. | % of all in treatment | Male (%) | Female (%) |
|---|
| 18-29 |
49 |
12% |
10% |
16% |
6,928 |
9% |
9% |
10% |
| 30-39 |
90 |
23% |
23% |
22% |
17,901 |
23% |
23% |
24% |
| 40-49 |
124 |
31% |
31% |
32% |
22,244 |
29% |
29% |
29% |
| 50-59 |
96 |
24% |
26% |
22% |
20,050 |
26% |
27% |
25% |
| 60+ |
35 |
9% |
9% |
8% |
9,617 |
12% |
12% |
12% |
| Source: PHE/NDTMS, Adults - alcohol commissioning support pack 2022-23: key data |
Drinking levels
Most people who require structured treatment for alcohol dependence will be drinking at higher risk levels. Drinking levels can be used as a rough proxy for level of dependence and levels of alcohol health risk. An indication of drinking levels in treatment may be useful in understanding which groups of adults are receiving treatment and whether those with the highest levels of harm are receiving effective interventions.
There is a strong association between levels of consumption and severity of dependence but they are not equivalent. For example, women are likely to become dependent at lower levels of consumption than men.
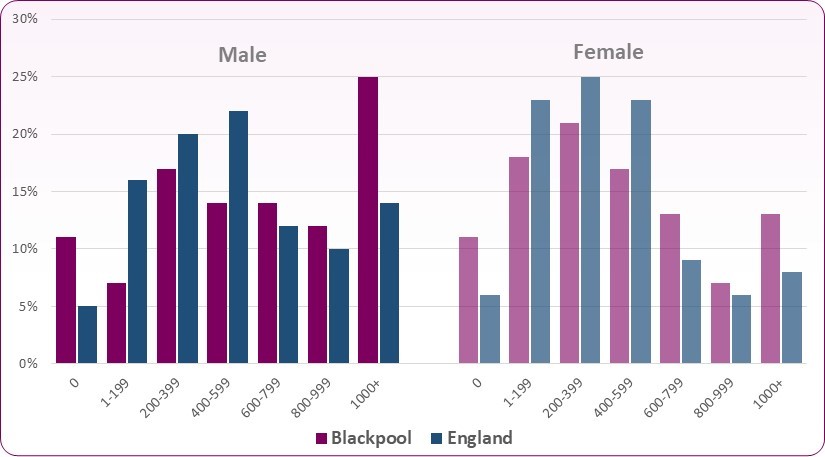
Figure 22 shows that for those entering treatment in Blackpool, they are drinking at significantly higher levels in the 28 days prior to commencing treatment than is seen nationally. Over a fifth of adults (25% of males and 13% of females) entering treatment are drinking in excess of 1,000 units per week, this is almost double the national average of 11%.
Figure 22: units consumed in the 28 days prior to entering treatment, Blackpool and England, 2020/21
 Source: PHE/NDTMS, Adults - alcohol commissioning support pack 2022-23: key data
Source: PHE/NDTMS, Adults - alcohol commissioning support pack 2022-23: key data
Clients who are parents/carers and their children
Research suggests that children experience negative outcomes as a result of their parents’ alcohol use, even amongst moderate drinkers.15
Data from NDTMS shows the number of alcohol only clients who entered treatment in 2020/21 who live with children and the stated number of children who live with them. Across Blackpool, 15% of alcohol clients in treatment had parenting responsibilities, this is lower than the national average of 24%. Many more women in treatment live with their child than men in treatment, 22% in comparison to 11%. 23% of clients in treatment and in contact with their children have early help or children’s social care involvement, a proportion similar to the national picture.
Figure 23: Alcohol only clients who are parents/carers by parental status, 2020/21
| | Blackpool | England |
|---|
| Parental status | No. | % of new presentations | Male (*) | Female (%) | No. | % of new presentations | Male (*) | Female (*) |
|---|
| Parents living with children |
39 |
14% |
9% |
22% |
11,626 |
22% |
17% |
29% |
| Other contact living with children |
<5 |
1% |
2% |
0% |
1,222 |
2% |
3% |
2% |
| Parents not with children |
37 |
13% |
15% |
11% |
9,389 |
18% |
20% |
15% |
| Not a parent/no contact with children |
195 |
70% |
74% |
64% |
28,974 |
55% |
58% |
51% |
| Missing/Incomplete |
<5 |
1% |
1% |
3% |
1,009 |
2% |
2% |
2% |
| Source: PHE/NDTMS, Adults - alcohol commissioning support pack 2022-23: key data |
Figure 24: Children living with adults entering alcohol only treatment, 2020/21
| | Blackpool | % of children by adult sex | England | % of children by adult sex |
|---|
| | Total adults | Male (*) | Female (*) | Total adults | Male (*) | Female (*) |
|---|
| Number of children living with alcohol client adult |
75 |
51% |
49% |
22,681 |
47% |
53% |
| Source: PHE/NDTMS, Adults - alcohol commissioning support pack 2022-23: key data |
Research has shown a number of barriers that women either experience or expect when seeking treatment.16 These include:-
-
- Caring responsibilities for children and fear of losing them
- Child custody arrangements
- Being dishonest with themselves about how serious the problem is
- Denial and minimisation of use, from which a health trigger may prompt the accessing of support
- Lack of knowledge re: options
- Inaccurate ideas about treatment
- Societal and self-stigma
- Economic issues and/or stigma
- Responsibilities, children, work, lack of free time
- Waiting times, many women feel they need immediate support before the moment passes
Blackpool Alcohol Strategy 2019-2022  (1.0MB) sets out the strategic priorities for local partners in tackling alcohol-related harm in Blackpool over the next three years
(1.0MB) sets out the strategic priorities for local partners in tackling alcohol-related harm in Blackpool over the next three years
The Blackpool Community Safety Plan, 2022-2025 sets out the analysis of crime, disorder and substance misuse and has identified the priorities that are of greatest threat to local people as well as where successful interventions will improve the quality of life in Blackpool.
The Blackpool Cumulative Impact Assessment 2021 relates to on and off licenced premises applications for the sale or supply of alcohol and was introduced as a tool to limit the growth of licensed premises in problem areas.
HM Government, The Government's Alcohol Strategy, March 2012
Home Office, Modern Crime Prevention Strategy, March 2016 - outlines the Government's plans for making the night time economy safe so people can consume alcohol safely without fear of becoming a victim of alcohol-related crime or disorder, enabling local economies to grow.
NICE guidance [PH24] Alcohol-use disorders: prevention covers alcohol problems among people over 10. It aims to prevent and identify such problems as early as possible using a mix of policy and practice, June 2010.
NICE Quality standard [QS83] Alcohol: preventing harmful use in the community covers preventing and identifying alcohol problems in the community. It includes policy and practice approaches to prevent harmful alcohol use in adults, young people and children. It is particularly relevant to local authorities, the police, and schools and colleges. It describes high-quality care in priority areas for improvement, March 2015.
The Public Health Burden of Alcohol and the Effectiveness and Cost-Effectiveness of Alcohol Control Policies. This evidence review looks at the impact of alcohol on the public health and the effectiveness of alcohol control policies, December 2016.
PHE, Health matters: harmful drinking and alcohol dependence provides information on the harmful impact of alcohol and focuses on alcohol dependence.
The following recommendations are from the Blackpool Alcohol Strategy 2019-2022:
-
- Priority 1: Reduce the prevalence of harmful drinking in Blackpool
- Priority 2: Reduce the impact of harmful drinking on communities in Blackpool
The measures to be used to achieve these priorities are to:
-
- Improve the population’s awareness of the Chief Medical Officer’s alcohol guidelines, alcohol-related harm and harm reduction.
- Provide targeted interventions to prevent alcohol misuse in those populations particularly at risk.
- Provide early help and interventions for people affected by harmful drinking.
- Provide evidence-based effective treatment for alcohol misuse that is accessible to all.
- Ensure that alcohol is sold and consumed responsibly.
- Advocate for changes in national policy and practice to reduce alcohol-related harm and better protect our population.
PHE, Health matter: harmful drinking and alcohol dependence, January 2016
OHID, COVID-19 Health Inequalities Monitoring for England (CHIME), November 2021
Blackpool Community Safety Plan, 2022-2025
NICE Guidance [PH24] Alcohol-use disorders: prevention, June 2010 (guidance is currently in the process of being updated)
DH, UK Chief Medical Officers' Low Risk Drinking Guidelines, August 2016
Bellis, M. A., Highes, K., Nicholls, J., Sheron, N., Gilmore, I. and Jones, L. (2016) The alcohol harm paradox: using a national survey to explore how alcohol may disproportionately impact health in deprived individuals, BMC Public Health, 16:1
Office for Health Improvement & Disparities, Local Alcohol Profiles for England.
NHS Digital, Hospital Admitted Patient Care Activity: 2020/21, by CCG of responsibility
Institute of Alcohol Studies, Violence and crime [Accessed March 2022]
Alcohol related crime is "any notifiable offence (crime) where it is perceived, by the victim or any other person, that the effects of alcohol consumption on the offender or victim was an aggravating factor", Home Office Counting Rules for Recorded Crime, Counting rules crime flags, April 2018
Institute of Alcohol Studies, Alcohol, domestic abuse and sexual assault, September 2014
PHE ADDER report for Blackpool – alcohol and non-opiate metrics from NDTMS
PHE – Adults Alcohol Commissioning Support Pack 2022-23: Key Data. Planning for alcohol harm prevention, treatment and recovery in adults: Blackpool.
NHS Digital, Health Survey for England 2018, Adult’s health-related behaviours, December 2019
] Institute of Alcohol Studies, One in three children report negative outcomes from parents’ drinking, November 2019
] Gremeax, L. Roets, G. Schamp, J. Simonis, S. Vanderplasschen, W. (2021) Research Report – Women’s Views on Barriers and Facilitators for seeking Alcohol and Drug Treatment in Belgium: Nordic Studies on Alcohol and Drugs Vol. 38 (2) 175-189. SAGE